Anaerobic Culture Media's Crucial Role in Diagnosing Unique Gas Gangrene Case
Rare Necrotizing Infection after Surgery Leads to Fatal Sepsis
Clostridial gas gangrene (GG) is an unusual but fast-spreading necrotic infection of soft tissue resulting in high mortality rates. GG, or clostridial myonecrosis, is a life‐threatening soft tissue infection caused by anaerobic, spore‐forming Clostridium subspecies (4). Up to 70% of cases of Clostridial gas gangrene (GG) are attributed to trauma, with additional predisposing conditions including bowel and biliary tract surgery, intramuscular injection, retained placenta, and intrauterine fetal death. Clostridium perfringens is the causative agent in nearly 80% of these infections, often associated with extensive penetrating trauma. (4)
Additional pathogens include Clostridium septicum, Clostridium novyi, Clostridium histolyticum, and Clostridium sordelli, the latter of which is commonly found in a gynecological context. (4)
Postoperative infections
Though rare, a 2020 case report published in Frontiers in Surgery shares the complete timeline of a 65-year-old male patient who died from a necrotizing infection after laparoscopic rectal cancer surgery.
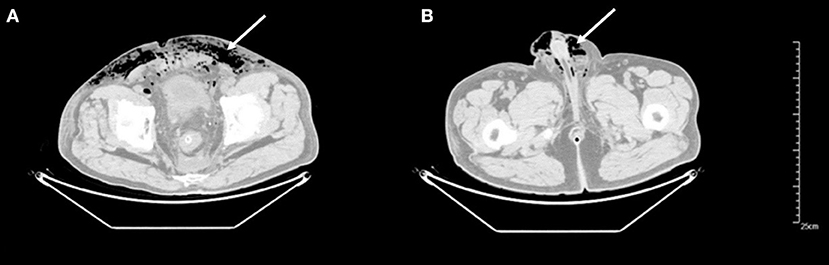
Postoperative infections are one of the most common complications in general surgery, and rates have been reduced with the routine administration of perioperative antibiotics (1). GG is reportedly more common after penetrating trauma or major surgery and is rarely reported without obvious predisposing events, such as edema, fever, malaise, and pain. Previous documents have only reported gas gangrene once after an open rectal surgery or laparoscopic cholecystectomy (2, 3). However, the authors of the case documented in the Frontiers in Surgery report say this is the first case of GG of the pelvic wall, after laparoscopic resection for rectal cancer, occurred.
Twenty-four hours after surgery, the patient started complaining of incisional pain in his lower abdomen. The following night the patient’s pain intensified and his condition continued to deteriorate. The patient was transferred to the intensive care unit where his healthcare team administered antibiotic therapy with meropenem, provided IV fluids, and high-oxygen flow treatments. Unfortunately, ten hours later, just two days post-op, he went into septic shock and was declared deceased.
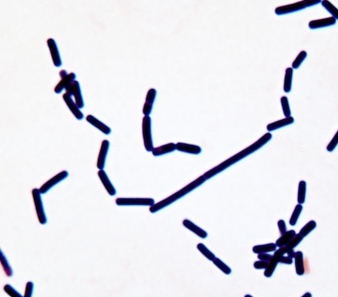
The GG diagnosis for this patient was difficult due to a number of reasons, including very acute onset, rapid progression of symptoms, limited time, and underlying health issues. Examination of discharge from the patient’s incision revealed infiltrated leukocytes and Gram-positive bacilli. The microbiologist concluded that the Gram-positive bacilli were most likely anaerobes, and the specimen was promptly cultivated on an anaerobic medium. The health care team also sent peripheral blood samples to identify the bacilli via next-generation sequencing (NGS). Subsequently, the peripheral blood sample confirmed the diagnosis of GG.
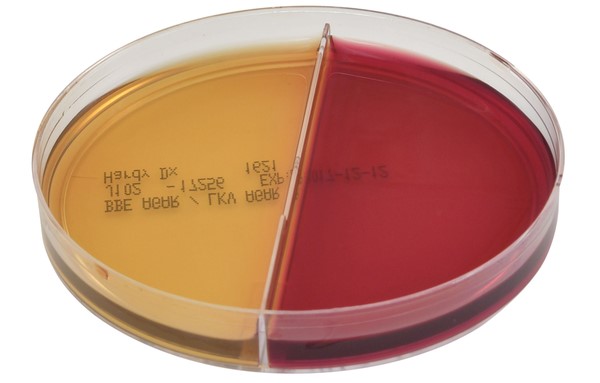
Anaerobic bacterial culture and frozen-section tissue biopsy are considered the gold standard of GG diagnosis. Cultures can then be identified using mass spectrometry (MALDI-TOF). According to the authors of the 2022 report, anaerobic culture of tissue or discharge is of, “great diagnostic value, especially when necrotizing fasciitis or GG is suspected.”
Hardy Diagnostics offers a complete line of pre-reduced anaerobic media:
When it comes to anaerobic, microaerophilc, and capnophilic growth atmospheres, Hardy has you covered. AnaeroGRO™ packets contain pre-reduced, nitrogen-flushed, media with a desiccant and an oxygen scavenger for the best recovery of anaerobic bacteria.
All AnaeroGRO™ plated media is provided in standard 15x100mm monoplates or biplates. Room temperature storage and ready-to-use right out of the pouch eliminates prereduction prep time of conventional media plates for anaerobes.
Download our FREE Anaerobic Microbiology Catalog

Contact us for additional support
1.Leaper D, Burman-Roy S, Palanca A, Cullen K, Worster D, Gautam-Aitken E, et al. Prevention and treatment of surgical site infection: summary of NICE guidance. BMJ. (2008) 337:a1924. doi: 10.1136/bmj.a1924
PubMed Abstract | CrossRef Full Text | Google Scholar
2.Bath M, McKelvie M, Canna K. Rare postoperative complication: Clostridium perfringens septic shock following elective abdominal surgery. BMJ Case Rep. (2017) 2017:bcr2017221980. doi: 10.1136/bcr-2017-221980
PubMed Abstract | CrossRef Full Text | Google Scholar
3.Harmsen AM, van Tol E, Giannakopoulos GF, de Brauw LM. Clostridial gas gangrene of the abdominal wall after laparoscopic cholecystectomy: a case report and review. Surg Laparosc Endosc Percutan Tech. (2016) 26:278–81. doi: 10.1097/SLE.0000000000000294
PubMed Abstract | CrossRef Full Text | Google Scholar
4. Leiblein M, Wagner N, Adam EH, Frank J, Marzi I, Nau C. Clostridial Gas Gangrene - A Rare but Deadly Infection: Case series and Comparison to Other Necrotizing Soft Tissue Infections. Orthop Surg. 2020 Dec;12(6):1733-1747. doi: 10.1111/os.12804. Epub 2020 Oct 4. PMID: 33015993; PMCID: PMC7767692.
Meet the author

CLINICAL PRODUCT MANAGER at HARDY DIAGNOSTICS
Megan Roesner, B.A. Journalism and Mass Communications
Megan is a seasoned writer and marketing professional who comes from a background in television journalism, followed by fifteen years leading mulitple hospital marketing and communications teams with the largest not-for-proft health system in the U.S. Megan has won numerous tv, writing and marketing awards and is a member of a number of professional public relations and marketing associations. Her passion for continuous professional challenges and life-long learning led her to Hardy Diagnostics. Megan is proud to work amongst a wonderful marketing team surrounded by experienced microbiologists and scientists who constantly push for the latest and greatest products to help diagnose and detect disease. In her current role, Megan is in charge of product development and marketing Hardy's clinical category which encompasses hospitals and health systems, clinics and research institutions, higher education and veterinary diagnostics. In her free time, Megan enjoys being a mom to her two very active boys, cats, a dog, a very old goldfish and 24 chickens.




