Carbapenem-Resistant Enterobacterales and the key to rapid phenotypic detection

Carbapenem-resistant Enterobacterales (CRE) refers to a group of bacteria within the Enterobacterales order that have developed resistance to carbapenem antibiotics. Carbapenems are a class of broad-spectrum antibiotics used as a last-resort treatment for serious infections caused by multi-drug-resistant bacteria.
Enterobacterales include pathogens such as Escherichia coli, Klebsiella pneumoniae, Enterobacter spp., and Serratia spp. When these bacteria become resistant to carbapenems, treating the infections they cause becomes significantly more challenging.
Resistance to carbapenems typically occurs due to the production of enzymes called carbapenemases, which break down the antibiotics, rendering them ineffective. CRE infections can lead to severe complications, including bloodstream infections, pneumonia, and wound infections. These infections are often associated with healthcare settings and are especially problematic for patients with weakened immune systems or those undergoing invasive procedures.
Preventing and controlling CRE involves stringent infection control practices, judicious antibiotic use, and regular monitoring in healthcare settings to prevent the spread of these resistant bacteria.
In 2017, CRE caused approximately 13,100 infections in hospital patients and resulted in around 1,100 deaths in the United States¹. Invasive CRE infections have an estimated mortality rate of up to 50%, making it imperative to quickly and accurately identify whether a pathogen is producing carbapenemase and, if so, determine the type.
Different carbapenemase enzymes require specific antibiotic regimens, and some enzymes can spread more easily through hospitals or hospital networks, contributing to the epidemic spread of antimicrobial resistance genes.
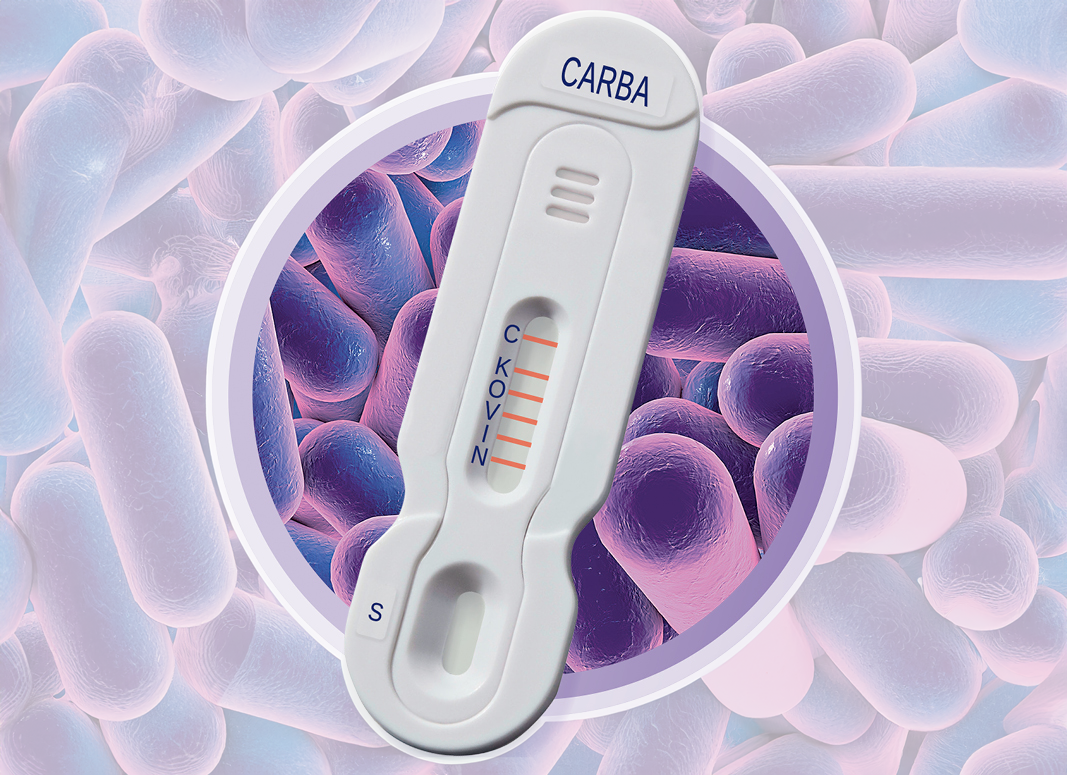
Only NG-Test® CARBA 5 can provide these critical answers.
Hardy Diagnostics is the exclusive distributor in the USA of the NG-Test® CARBA 5, the only FDA-cleared, rapid in vitro multiplex immunochromatographic assay for the phenotypic detection of the five most common carbapenemases: KPC, NDM, VIM, OXA-48-like, and IMP.
This device delivers phenotypic test results in 15 minutes using colonies from HardyCHROM™ CRE agar, blood agar, or MacConkey agar. With about one minute of hands-on time and results in 15 minutes per test, CARBA 5 naturally integrates into any laboratory workflow.
Unlike molecular methods, CARBA 5 detects the presence of the big five carbapenemase enzymes, which is crucial for aiding therapeutic decisions. Furthermore, CARBA 5 has been shown to detect several carbapenemase variants that predicate PCR methods may miss.
NG-Test® CARBA 5 can replace molecular detection methods. Molecular tests require specialized technician training, are expensive per test, and can take two to three hours to provide a result. Additionally, molecular assays detect the presence of specific genes but do not indicate whether the gene is being expressed. NG-Test® CARBA 5 detects and differentiates carbapenemases produced by microorganisms, delivering a phenotypic result.
The Infectious Disease Society of America (IDSA) guidelines strongly recommend that clinical microbiology laboratories pursue carbapenemase testing to identify the presence of specific carbapenemases produced by CRE isolates².
mCIM and eCIM assays detect and differentiate between the two major groups of carbapenemases: serine beta-lactamases (such as KPC and OXA-48-like) and metallo-beta-lactamases (such as VIM, IMP, and NDM). However, CIM tests are unable to further differentiate specific enzymes. Additionally, in the mCIM and eCIM assays, serine beta-lactamases can mask metallo-beta-lactamases if both enzymes are co-produced.
The Carba NP test, another phenotypic assay, has limitations similar to those of the CIM test in that it cannot differentiate between specific carbapenemases.
CARBA 5 addresses this issue by detecting and differentiating multiple carbapenemases in a single assay.
Since 2018, CARBA 5 has been the subject of more than 100 peer-reviewed publications and posters. Published results from over 30 countries, with more than 8,000 isolates tested, support a sensitivity of 98.4% and a specificity of 99.6%. Additionally, a multicenter US clinical trial resulted in a sensitivity of 100% and specificity of 100% after discrepant analysis. Read more of the evaluation here.
Footnotes:
- CDC. Antibiotic Resistance Threats in the United States, 2019. Atlanta, GA: U.S. Department of Health and Human Services, CDC; 2019.
- Infectious Diseases Society of America (IDSA) Practice Guidelines on Antimicrobial Resistance.

Meet the author

CLINICAL PRODUCT MANAGER I at HARDY DIAGNOSTICS
Megan Roesner, B.A. Journalism and Mass Communications
Megan is a seasoned writer and marketing professional who comes from a background in television journalism, followed by fifteen years leading mulitple hospital marketing and communications teams with the largest not-for-proft health system in the U.S. Megan has won numerous tv, writing and marketing awards and is a member of a number of professional public relations and marketing associations. Her passion for continuous professional challenges and life-long learning led her to Hardy Diagnostics. Megan is proud to work amongst a wonderful marketing team surrounded by experienced microbiologists and scientists who constantly push for the latest and greatest products to help diagnose and detect disease. In her current role, Megan is in charge of product development and marketing Hardy's clinical category which encompasses hospitals and health systems, clinics and research institutions, higher education and veterinary diagnostics. In her free time, Megan enjoys being a mom to her two very active boys, cats, a dog, a very old goldfish and 24 chickens.