Fluoroquinolone Resistance and Screening Methods

Fluoroquinolones have been the staple of antimicrobial therapy since the launch of the flagship representative "Ciprofloxacin" by Bayer in the early 1980s.
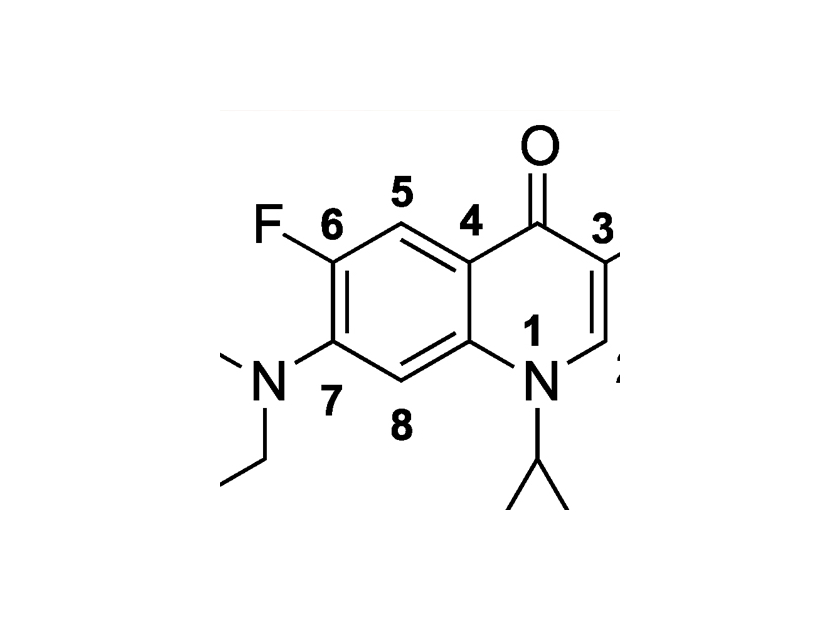
Fluoroquinolones have a fluorine atom attached to the core quinolone molecular ring and this modification results in a class of broad-spectrum bactericidal agents that show increased stability and potency against both Gram negative and Gram positive organisms.
 In the years since its introduction, many other fluoroquinolones have been cleared for use, such as gemifloxacin, levofloxacin, moxifloxacin, and ofloxacin, among others. As predicted, resistance to fluoroquinolones has increased in the last decade, as the majority of fluoroquinolones were introduced in the late 1990s. For instance, in large surveillance programs like SENTRY, data from 2013 to 2016 show the resistance rates at 15.6% and 18.6% for general Enterobacteriaceae and
In the years since its introduction, many other fluoroquinolones have been cleared for use, such as gemifloxacin, levofloxacin, moxifloxacin, and ofloxacin, among others. As predicted, resistance to fluoroquinolones has increased in the last decade, as the majority of fluoroquinolones were introduced in the late 1990s. For instance, in large surveillance programs like SENTRY, data from 2013 to 2016 show the resistance rates at 15.6% and 18.6% for general Enterobacteriaceae andAntimicrobial Agents and Chemotherapy publication by Bidell et al., the rate of resistance in Escherichia coli strains from hospital-associated urinary tract infections range from 25% to 43% (ref. 2). These recent data certainly support the importance of screening for non-susceptible isolates in patients prior to administering the drug for treatment.
 Generally, resistance to fluoroquinolones occurs through step-wise mutations, which are a series of point mutations that occur over time in the gyrase or topoisomerase gene that alter the bacterial enzyme structure to make the fluoroquinolone less effective or ineffective at binding and disabling the enzyme. When a new fluoroquinolone is administered, it may be effective at killing the bacteria at first. However, point mutations that lead to a beneficial change in enzyme structure are selected for which facilitates resistance against the new drug. Each new fluoroquinolone presents a new selective pressure that a previous fluoroquinolone may not have presented. However, mutations can accumulate one at a time or in a step-wise manner, leading to increasing fluoroquinolone resistance with each successful mutation (ref. 3).
Generally, resistance to fluoroquinolones occurs through step-wise mutations, which are a series of point mutations that occur over time in the gyrase or topoisomerase gene that alter the bacterial enzyme structure to make the fluoroquinolone less effective or ineffective at binding and disabling the enzyme. When a new fluoroquinolone is administered, it may be effective at killing the bacteria at first. However, point mutations that lead to a beneficial change in enzyme structure are selected for which facilitates resistance against the new drug. Each new fluoroquinolone presents a new selective pressure that a previous fluoroquinolone may not have presented. However, mutations can accumulate one at a time or in a step-wise manner, leading to increasing fluoroquinolone resistance with each successful mutation (ref. 3). Fluoroquinolones are widely administered for urinary tract infections, pre- and post-prostate biopsy, and hospital or community acquired infections that show multi-drug resistance. However, the use of fluoroquinolones has been cautioned against as there have been cases linked to devastating side effects that involve the central nervous system and tendon rupture (especially the Achilles tendon).
Fluoroquinolones are widely administered for urinary tract infections, pre- and post-prostate biopsy, and hospital or community acquired infections that show multi-drug resistance. However, the use of fluoroquinolones has been cautioned against as there have been cases linked to devastating side effects that involve the central nervous system and tendon rupture (especially the Achilles tendon).

Meet the author

SENIOR TECHNICAL SERVICES AND R&D MANAGER at HARDY DIAGNOSTICS
Anna Klavins, RAC-Devices, B.S Cellular and Molecular Biology
Anna Klavins is the Senior Technical Services and R&D Manager at Hardy Diagnostics where she oversees the Research and Development, Design and Development, Quality Control, Technical Support, and Performance Studies teams. She earned a Molecular and Cellular Biology B.S. degree from Cal Poly San Luis Obispo while playing for the Division I NCAA women’s tennis team. Since joining Hardy Diagnostics in mid-2016, she has authored sixteen FDA 510(k) submissions for class II microbiology in vitro diagnostic devices. She has published in the Journal of Clinical Microbiology and the Journal of AOAC INTERNATIONAL, as well as presents in vitro diagnostic device performance evaluation results annually at global scientific conferences such as ASM Microbe, the AOAC Annual Meeting, and the International Association of Food Protection annual meeting. She is an advisor to the Joint CLSI-EUCAST Working Group and has earned the RAC-Devices certification.