Puzzling Case Solved by Next Generation Sequencing

Case history of a brain destroying amoeba...
A 56-year old man presented with transient coma, nausea, and vomiting when he visited the local hospital. There were no visible abnormalities observed in the MRI and his CSF pressure on the second day of illness was 275mmH2O.
Despite receiving symptomatic treatment, the patient developed drowsiness and a severe headache.
A neurological examination showed hypersomnia (excessive sleepiness), stiff neck, a positive Kernig sign (not being able to extend the knees beyond 90 degrees without pain), and normal muscle strength in the limbs.
Further, he had dark red lesions located on both forearms. He had not been on any recent travel, and had no history of freshwater swimming. There was also no report that he had consumed undercooked meat or unpasteurized dairy products. He had worked in a garbage dump for about two years prior to his illness. Bacterial and fungal cultures as well as cytology of the CSF were all negative.
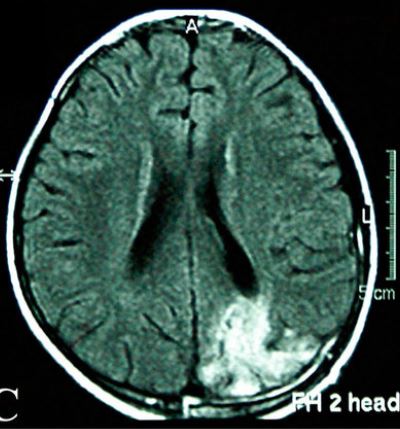
Ultimately, the patient was diagnosed with CNS infection and treated accordingly but his condition worsened on day 14 of onset with development of lethargy, urinary and fecal dysfunction, and weakness of both lower limbs. MRI of both brain and several spinal cord segments showed abnormal signals (MRI from a different patient with Balamuthia is shown above).
It took a consultation with infectious disease specialists and two NGS (Next-generation Sequencing, pictured below) results to finally diagnose the man with encephalomyelomeningitis caused by Balamuthia mandrillaris. After receiving a combination of various antimicrobials, his prognosis worsened and he died 30 days after the disease onset. (1)
When all other tests failed, NGS made the diagnosis.


Balamuthia mandrillaris is a free living ameba naturally found in the environment (photo above). It lives freely in soil around the world and may also be present in fresh water.
Gardening, playing with dirt, or breathing in soil carried by the wind might increase the risk of infection. It is able to infect anyone, including healthy people. Since its first discovery in 1986, about 200 cases of infection have been reported worldwide, making B. mandrillaris infections extremely rare. (2) This organism can cause a rare and serious infection of the brain called granulomatous amebic encephalitis (GAE) which is fatal in 90% of cases.
Balamuthia amebas are thought to enter the body when soil containing the organism comes in contact with skin wounds and cuts, or when dust containing Balamuthia is breathed into the lungs. After initial exposure, the amebas can travel to the brain and cause GAE. It can take weeks to months to develop the first symptoms of Balamuthia GAE after initial exposure.
According to reports, B. mandrillaris infections can manifest in two main ways.
The first is more common in the United States and presents as encephalitis without skin lesions.
The second is more commonly seen in China and Peru where the skin is usually involved first and then encephalitis develops gradually. The skin lesions usually appear as painless plaques or ulcers and are commonly seen in the center of the face but may also appear on the trunk, hands, and feet. (1) In the case of the 56 year old patient, a pathological examination of the lesions on his forearms was not done and therefore it is not confirmed if this case was a cutaneous manifestation of B. mandrillaris infection.
Non-specific symptoms are the main reason that diagnosis of B. mandrillaris can be very difficult. NGS technology can provide a rapid, early etiologic diagnosis without the need for a local brain biopsy.
Although the mortality rate is high for B. mandrillaris infections, early diagnosis and treatment will offer the best chances of survival.
Written By Alani Vasquez - R&D Manager at Hardy Diagnostics
Meet the author

R&D MANAGER at HARDY DIAGNOSTICS
Alani Vasquez
Alani Vasquez received her B.S. in Microbiology from Cal Poly San Luis Obispo. She began working for Hardy Diagnostics in 2014 as an R&D Technician working on new culture media formulations. Alani now manages R&D projects and strives to build a team of innovative thinkers and problem solvers. As the manager of R&D, her goal is to carve a future for Hardy Diagnostics through innovation and technology. In her spare time, Alani enjoys spending time in her garden, making sourdough bread, and caring for her many animals including chickens, dogs, and a cat.